For those of you who were not able to visit our poster at the 2023 ASHA Convention, we will summarize the results below. Click here to read about our hypothesis and research design.
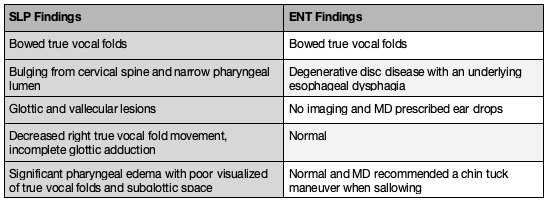
Of the 1,003 residents who received FEES, 58 residents were identified as having laryngeal or pharyngeal abnormalities. Of note, these were anatomical findings that were outside of normal variants or general inflammation. Of those 58 residents, only 17 were scheduled for ENT appointments. Of those 17, only five residents actually attended appointments. Of the five who attended the appointments, the results were interesting, see table below.
The primary clinicians reported that the following factors contributed to lack of ENT follow-up:
- Resident discharge from facility prior to scheduling outside appointment
- Lack of primary SLP response to follow-up inquiry
- Resident hospitalization
- Postponement due to illness or being ventilator dependent
- Resident or MD declined the work up due to advanced age, other co-morbidities, and/or POA discussion
As onsite FEES clinicians, our ability to accurately identify anatomical abnormalities and make appropriate referrals can help guide a person’s plan of care. That being said, there are clearly barriers to access. By providing relevant results to the patient and the medical team, we open up the discussion to allow the resident and their providers to make educated decisions on whether to pursue follow-up.
The outcomes for those who did receive access to the ENT consultation were interesting as the ENT findings and recommendations did not appear to match the reason for the consultation. There needs to be further discussion on incidental laryngeal findings and subsequent recommendations for follow-up with ENT services. It may be more appropriate to specify a laryngology specialization when making these referrals; however, this may further complicate access, especially in rural areas.
Limitations in this study include small sample size and limited access to resident records from the ENT visit. Longitudinal follow-ups with patients upon discharge are needed, along with studies to identify barriers to access to consultants for patients in these settings.