Both FEES and MBSS are excellent tools to evaluate oropharyngeal swallow function. Each tool has its strengths and limitations. A strength of MBSS is that it allows visualization of the entire swallow event and can identify deficits beyond the pharyngoesophageal segment. An important strength of FEES is the ability to identify laryngeal abnormalities. This is essential, as many patients may never have direct visualization of this part of the anatomy without having participated in a FEES exam. This is especially important in patients who have experienced prolonged intubation where the likelihood of laryngeal injury may be increased. A study published in 2021 demonstrated that of the 75 patients who failed a nursing swallow screen and were referred for FEES, 29 were identified to have a laryngeal pathology. One of those 29 was later shown to have cancer. (Pazak, et al 2021)
What is the importance of Fees?
Why is this important? As mentioned above, FEES is possibly the only opportunity for visualization of the upper airway. These patients with laryngeal pathologies might otherwise go unnoticed. And for that 1 person out of 29 who was found to have a malignancy, this is crucial and potentially life-saving. As FEES clinicians, it is essential for us to be familiar with laryngeal variations versus laryngeal pathologies, which is why CSP’s clinicians undergo intensive training to ensure we are proficient in identifying abnormalities and recommending further consultation as appropriate. Here is one patient’s story.
A long-term care resident was referred to SLP for increased coughing with meals. This patient had a history of alcohol and tobacco dependence and COPD.
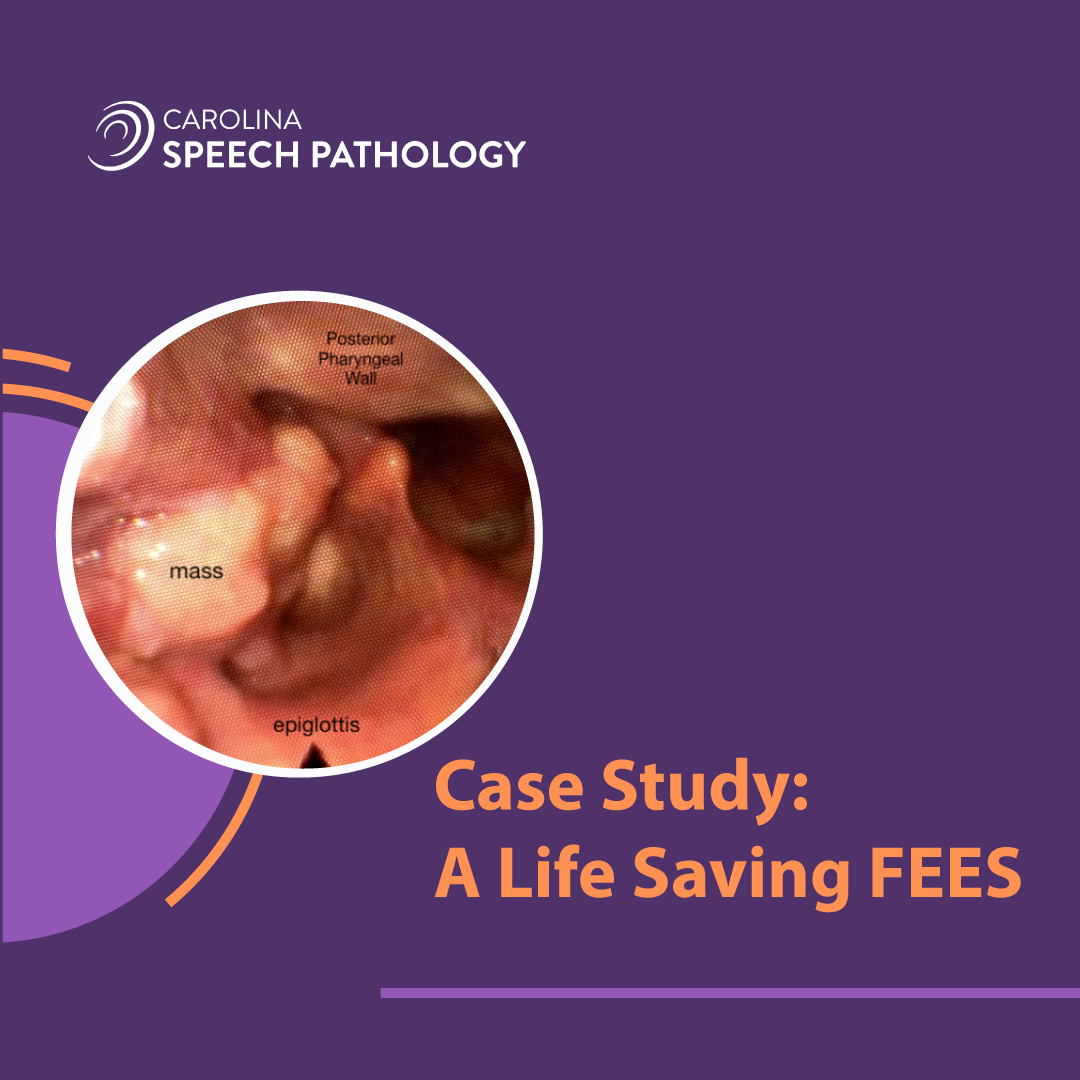
The FEES was completed and the patient was found to have a large, lumpy mass from the R pharyngeal wall encroaching into the patient’s hypopharynx and laryngeal vestibule. This obliterated the view of the R side of the patient’s larynx. It was suspected that perhaps tethering or blockage from the observed mass along with suspected diminished hyolaryngeal elevation/excursion led to minimal epiglottic inversion and incomplete laryngeal vestibule closure. Airway invasion was noted before and during the swallow with thin and mildly thick liquids. Patient demonstrated a reflexive clearing response with thin, but not mildly thick textures. The exam was terminated after testing only pureed, mildly thick liquids, and thin liquids due to patient not wanting to trial solids.
Recommendations and Follow-Up Post FEES:
Recommendations:
- ENT consultation as soon as possible to address large mass on R side of hypopharynx which potentially could compromise airway
- Consider continuing pureed with thin liquids with regular oral care to minimize risk of developing aspiration pneumonia.
Follow-Up:
We checked back in with this patient’s primary SLP approximately two months later. SLP reports the patient was sent to ENT. The mass was identified as cancer, stage 4A squamous cell cancer of the R lateral aspect of the larynx involving the R aryepiglottic fold. Patient is awaiting follow-up with Oncology for treatment. SLP reports the patient is in good spirits, but that his breathing has become more labored and audible. The SLP has promised to continue to keep us updated and in the meantime we are sending well wishes his way.
If you have questions or want to schedule a FEES, visit our website today to learn more. Carolina Speech Pathology is the premier provider of onsite swallowing studies. Our onsite swallowing evaluations equip SLPs with a more accurate diagnosis so they can move their patient’s plan of care forward, reduce hospitalizations and experience a better quality of life. View our COVID-19 update here.